In an article in the April 29 issue of the New England Journal of Medicine titled What's Keeping Us So Busy in Primary Care? A Snapshot from One Practice (pdf) Richard Baron analyzes his practices activities. What is surprising is the extent to which non-reimbursed activities are part of the general work.
The breakdown of services averaged per visit and physician and by patient is shown below

Telephone calls averaged 23.7 per physician per day with close to 80% being handled directly by physician. Even running at peak efficiency with no time requirement to get to the phone, waiting on hold you can expect this to conservatively consume 2-3 minutes of time per day which equates to over an hour on phone calls per day. There were slightly fewer e-mails but the time taken to respond is likely to be a little longer to read and then respond. Add in prescription refills, laboratory reports and imaging and consultation reports and the time consumed for this ancillary activity has to be approaching 2-3 hours. The overhead of the system places an undue burden on primary care physicians and it is no surprise that medical school graduates are avoiding the field given the low reimbursement and declining compensation. As the author states in the summary:
Primary care practitioners (PCP) are better compensated than next closest - an MBA graduate but significantly less than specialists (and Cardiology is not the highest compensated specialty - AMGA Medical Group Compensation and Financial Survey pdf here). All this does not bode well for what is a the lynch pin in patient management and longitudinal relationships with patients. As noted in a recent posting in the Health care blog Why We Need Private Primary Care Doctors - aside from the basic need there is a clear economic justification that supports empowering and paying PCP's and attracting more physicians into this specialist area. And as Rob Lamberts points out points out
The solution from an overall cost standpoint is to give primary care physicians incentive to do what they should be doing in the first place: keep people healthy and away from hospitals. Any system that places too much value on procedures is going to fail at this, as the institutions and individuals who profit off of the procedures are going to fight for control of PCP’s. Independent PCP’s who profit from keeping people well are the best thing for a system.
Which reminds me of a point made some time back on Universal Healthcare - Pay While you are Healthy which cited age old system in China
Do you agree - do you have better ideas on how to make things better and what technology or processes can be applied or improved - let em know and leave your comments

The breakdown of services averaged per visit and physician and by patient is shown below

Telephone calls averaged 23.7 per physician per day with close to 80% being handled directly by physician. Even running at peak efficiency with no time requirement to get to the phone, waiting on hold you can expect this to conservatively consume 2-3 minutes of time per day which equates to over an hour on phone calls per day. There were slightly fewer e-mails but the time taken to respond is likely to be a little longer to read and then respond. Add in prescription refills, laboratory reports and imaging and consultation reports and the time consumed for this ancillary activity has to be approaching 2-3 hours. The overhead of the system places an undue burden on primary care physicians and it is no surprise that medical school graduates are avoiding the field given the low reimbursement and declining compensation. As the author states in the summary:
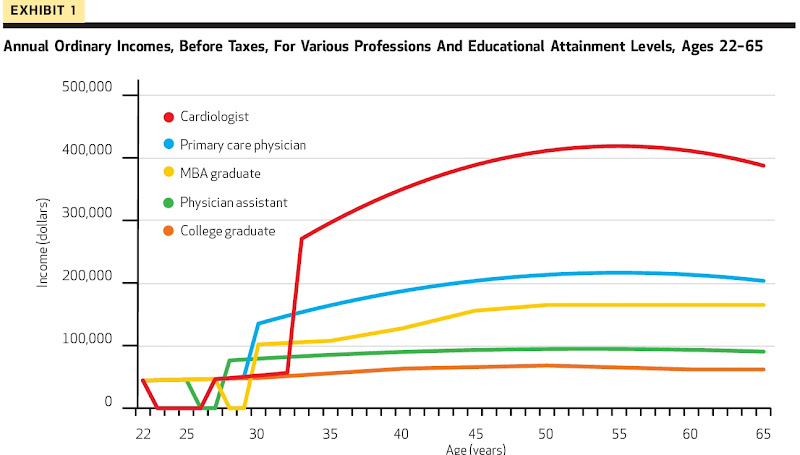
The core of primary care remains the longitudinal, trusted relationship with the patient, in which diagnostic skill, therapeutic understanding, and compassion come together for the benefit of the patient who seeks our help. Achieving that mission for patients with varying communication and computer skills is a daily challenge, even as our office faces a fragmented payment system and rapidly evolving technology. The work we describe arises from the needs of patients in a society that assigns many roles to physicians — from making diagnoses and providing treatment to ordering tests and filling out forms — and the practice must be organized to respond reliably. How and by whom the work is done is a continuing project of primary care redesign, dependent on both the skills of available non physician staff and the extent of information-technology support.Recent reviews of compensation compared the broad categories imply that while this compensation is not as good as specialist it is still better than many others. Healthaffairs reviewed compensation and asked: Can We Close The Income And Wealth Gap Between Specialists And Primary Care Physicians (full text requires subscription) but the chart showing compensation comparisons over time is helpful:

Primary care practitioners (PCP) are better compensated than next closest - an MBA graduate but significantly less than specialists (and Cardiology is not the highest compensated specialty - AMGA Medical Group Compensation and Financial Survey pdf here). All this does not bode well for what is a the lynch pin in patient management and longitudinal relationships with patients. As noted in a recent posting in the Health care blog Why We Need Private Primary Care Doctors - aside from the basic need there is a clear economic justification that supports empowering and paying PCP's and attracting more physicians into this specialist area. And as Rob Lamberts points out points out
The solution from an overall cost standpoint is to give primary care physicians incentive to do what they should be doing in the first place: keep people healthy and away from hospitals. Any system that places too much value on procedures is going to fail at this, as the institutions and individuals who profit off of the procedures are going to fight for control of PCP’s. Independent PCP’s who profit from keeping people well are the best thing for a system.
Which reminds me of a point made some time back on Universal Healthcare - Pay While you are Healthy which cited age old system in China
Hark back to days gone by in Chinese villages where the villagers paid the medicine man when they were healthy. When they fell ill they stopped paying until they were better and able to work againAnd as KevinMD originally said
Lifestyle matters. More doctors are entering the workforce seeking part-time jobs in order to maintain a family balance. By removing the administrative hassles from their plate, they can go back to focusing solely on practicing medicine and coming home at a reasonable hourThe way to do that is using technology that supports not hinders clinical work flow and clinical thinking. Incorporate new tools and communication methods into the process and acknowledge their value by including them in compensation structure.
Do you agree - do you have better ideas on how to make things better and what technology or processes can be applied or improved - let em know and leave your comments

No comments:
Post a Comment
Note: Only a member of this blog may post a comment.