Healthcare from the perspective of a clinician encompassing both the capture of the clinical viewpoint as well as the technology to help clinicians capture knowledge at the point of care
The thoughts expressed are my own and do not necessarily represent those of Nuance
The Panel "The Art of Medicine" Panel (part of the Art of Medicine campaign) took place yesterday from 9 - 11am at the Boston's W Hotel, 100 Stuart St, Boston, MA
Keith Dreyer, DO, PhD, FACR, Vice Chairman of Department of Radiology, Massachusetts General Hospital
Adam Landman, MD, MS, MIS, MHS, CMIO, Health Information and Integration at Brigham and Women's Hospital (@landmaad)
Steven J. Stack, MD, past chair of the American Medical Association (AMA); served on multiple federal advisory groups for ONC on HIT, practicing emergency physician
and at the far right moderated by Paul Weygandt, MD, JD, MPH, MBA, CCS, CPE, Vice President of Physician Services, Nuance Communications
And it was very well attended:
Today, physicians are struggling to serve their patients’ needs in a healthcare system that seems to work against them at every turn. While technology has the potential to vastly improve healthcare overall, issues remain when it comes to usability, data-entry and complementing patient care vs. competing with it.
In part 1 I have attempted to capture the underlying sentiments and thoughts form our panelists together with some thoughts on potential ways to help resolve these areas and problems.
The panel opened with the original Art of Medicine video:
The session was divided into several separate discussions - the first of which the Issues of today:
There has been an increasing burden placed on physicians to document more and more detail but no additional time to do this and in fact probably less and they struggle with the increasing information over load and the challenge of processing - As John Halamka put it:
"We need wisdom and today's #EHR make that hard to get from patient info to give me what I need now"
"3 petabytes of patient data...overwhelmed with data, we just need information, knowledge"
This is combined with the increasing regulations which the panel viewed as directly linked to the increasing need for HealthIT tools to help deal with these regulations. As Adam Landmaan put it the design of the EHR’s is based on the design focus and in the current fee for service health system is designed largely support the physicians to capture and document optimize for bill not for patient care
But I thought Keith Dreyer captured the sentiment well when he described technology as decreasing our ability to communicate
“I couldn't imagine dictating into a microphone in talking with my family "
And we are seeing declining capture off the patient’s story in the EHR
Some snapshots of ideas thoughts from our panelists included:
IT tools driving “note bloat” of information that is non-specific to the patient
Physicians need timely “wisdom” to positively effect patient care at the time of encounter
“Big bang” of government funding for EHR adoption has generated massive amounts of information that is, at present, unmanageable
At stage now of EHRs where they are “one size fits all,” so not customized to specific specialty/setting needs
Need to identify the smallest number of moving parts (IT tools) to facilitate patient care
Need for monolithic (“one size fits all”) IT solutions is driven by babel of nomenclature
Quality measures show that there is a problem, but not the causality
There was much more discussions and thoughts on solutions but one of the concepts that stood out for me was this one from Adam Landmaan straight out of the Television Reality show - copying the Shark Tank concept
That will be an interesting panel and team event and look forward to hearing the results
We need to return to the Art of Medicine and as one panelist put it:
People sought out Doctors in the past even when they actively hurt you and bled you
They did this because the doctor provided compassion and care that had the best intentions - they cared about their patient and the Art of Medicine
Physicians don’t act on business motives. They act on patient care motives.
You can see the #ArtofMedicine HashTag Social Media Statistics here and analytics here
Steven J. Stack, MD, past chair of the American Medical Association (AMA); served on multiple federal advisory groups for ONC on HIT, practicing emergency physician
Keith Dreyer, DO, PhD, FACR, Vice Chairman of Department of Radiology, Massachusetts General Hospital
Adam Landman, MD, MS, MIS, MHS, CMIO, Health Information and Integration at Brigham and Women's Hospital (@landmaad)
and moderated by Paul Weygandt, MD, JD, MPH, MBA, CCS, CPE, Vice President of
Physician Services, Nuance Communications
The panel is taking place this Thursday from 9 - 11am at the Boston's W Hotel, 100 Stuart St, Boston, MA. If you have not already you can register here: www.nuance.com/artofmedicine. The event is free of charge,
“If we want doctors to do better work, we need to give them better work to do.”
and to do that doctors have to engage in the design of these solutions and the clinical community and the #HealthIT world must address these issues:
Just as we can’t expect a patient with heart disease to know intrinsically to maintain a low-sodium diet, we can’t expect the healthcare industry to know how to fix everything unless we speak up and advocate for change (especially with the other loud voices of insurers and politicians speaking on “our behalf”)
Some solutions are not technical as this Tweet by "Dr K" @MedschoolAdvice)
Sitting down in room makes patients feel you've spent more time w/ them than if u stand whole time, even if u spent same time. So sit
— Dr. K (@medschooladvice) March 21, 2014
We have the rare opportunity to shape the future of healthcare infused with technology and I, for one, want to be part of developing a solution that helps the next generation of physicians offer that comforting touch as they deliver an even greater level of care to their patients
Download the Art of Medicine eGuide here and join me and the panelist on Thursday as they discuss they start to shape a better HealthIT future for everyone. I will be live tweeting from the panel (#ArtofMedicine) and will post a summary after the event.
I know I am biased as one of the lucky Google Glass Explorer as can be seen in this post from MedCity Watching for Wearables at #HIMSS14:
I think they are wrong and its not just Glass that will provide better more ready access to essential clinical data.
Not to say that the initial program like many launches have had their problems with early releases of technology not quite ready for prime time - remember the 1987 Apple Newton:
Mat Honan (one on the same “Epic Hack”) wrote a piece about his early experiences “My Year with Google Glass” that highlighted some early acceptance challenges
Glass is socially awkward
People get angry at Glass
Wearing Glass separates you
and I would add Glass interrupts normal conversations and social behavior - but that is all now and like the mobile phone I believe it will be come a natural part of our technical fabric. Think back to 2007 and how pulling out a phone in a meeting was frowned upon - now it seems part of the fabric of many of the meetings I attend.
But it was Mat’s commentary on the impact it had on his perception fo phones that really stuck out for me
Glass kind of made me hate my phone — or any phone. It made me realize how much they have captured our attention. Phones separate us from our lives in all sorts of ways. Here we are together, looking at little screens, interacting (at best) with people who aren’t here. Looking at our hands instead of each other. Documenting instead of experiencing.
From initial diagnosis through to surgical therapies, chemotherapy treatments and even end-of-life care, my job is to listen, assess and provide educated decisions that ultimately impact the health and wellness of another human being…. it’s my belief that when talking face-to-face with a patient about a care plan aimed at eradicating their body of a disease that threatens to take them away from their family, there’s no room for paper, computers and/or mobile devices. In these most intimate of conversations, the focus has always and must remain on the communication between the caregiver and the patient on the receiving end. That, in its purest essence, is what practicing the art of medicine is truly all about.
That’s not to say that Google Glass can solve this problem and in its current state and acceptance it might cause more challenges - but the potential is there to blend information access and capture into a physician patient interaction that remains all about the patient
Glass will provide improved access to essential clinical data to clinicians but as my friend Chuck Webster has pointed out on several occasions this is not just for clinicians. Patients are already accessing the internet in droves for clinical information, researching their conditions and that of their relatives and communities abound with resources and support for conditions from common to rare.
Before talking about some of the potential medical applications it is worth detailing the technology. Google Glass is basically a computer with 12Gb of memory attached to your head in the form of glasses. It has a heads up display with voice activation and has some apps that can be installed:
Facts
Google Glass is basically a computer attached to a pair of glasses
Google Glass has a display that is projected in front of the Right Eye that is a high resolution display equivalent of a 25 inch high definition screen from eight feet away
Google Glass has a camera that points forward and can take pictures (5MP) or video (720p) that is closely aligned with the view you see from your own eyes
Google Glass is voice activated using speech recognition to interact with the glass computer
Google Glass works best when connected to the internet
Google Glass Integrates with an Andorid Phone with a limited set of functions available for the iPhone
Google Glass has no built in illumination so pictures or video taken in dark conditions do not work well
The screen can be hard to see in bright light
There are many myths circulating:
Myths
If someone is wearing Google Glass they are recording me
False - The device is not set up to record continuously and will only record a video or photo based on an action by the wearer (either a spoken request
OK Glass, take a picture
or by pressing a button on the google glass device
Once Someone Has recorded something on Google Glass it is Publicly Posted
False - it requires an action on the part of the Glass owner to post the material to the internet otherwise it resides on the Google Glass device. It will be synchronized with the users Google+ account for automatic backup (much like photos are backed up from the iPhone to iCloud but like iCloud remain private to the user unless they elect to share them)
Google Glass is constantly capturing data and transmitting it to the Internet
False. Without an internet connection Google Glass simply stores any recorded information in the glass memory. And unless you have set it to record there is no data being captured
Google Glass tracks users and unsuspecting bystanders
False - Google Glass is not tracking or recording anything unless instructed to do so by the user
So who is using this technology, where are they using it and how are they using it in Healthcare. This article covered some of the early concepts and featured a short list of potential applications
Video sharing and storage: Physicians could record medical visits and store them for future reference or share the footage with other doctors.
A diagnostic reference: If Glass is integrated with an electronic medical record (EMR), it could provide a real-time feed of the patient’s vital signs.
A textbook alternative: Rather than referring to a medical textbook, physicians can perform a search on the fly with their Google Glass.
Emergency room/war zone care: As storied venture capitalist Marc Andreessen proposed in a recent interview, consider ”dealing with wounded patients and right there in their field of vision, if they’re trying to do any kind of procedure, they’ll have step-by-step instructions walking them through it.” In a trauma situation, doctors need to keep their hands free.
Helping medical students learn: As suggested by one blogger, a surgeon might live stream a live — and potentially rare — surgery to residents and students.
Preventing medical errors: With an electronic medical record integration, a nurse can scan the medication to confirm whether it’s the correct drug dose and right patient
In its simplest form just transmitting images in real time can offer some advantages for diagnosis - in Rhode Island they are planning on implementing Google Glass for the ED doctors to obtain real time consults with dermatologists.
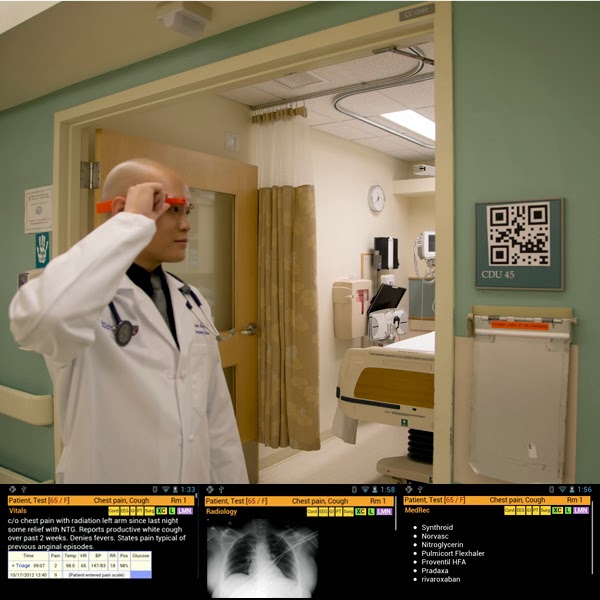
And this from Kareo showing a patient education application that records the physician patient interaction and then makes it available afterwards for additional review:
When a clinician walks into an emergency department room, he or she looks at [a] bar code (a QR or Quick Response code) placed on the wall. Google Glass immediately recognizes the room and then the ED Dashboard sends information about the patient in that room to the glasses, appearing in the clinician’s field of vision. The clinician can speak with the patient, examine the patient, and perform procedures while seeing problems, vital signs, lab results and other data.
And this concept by the way was top of everyone's wish list that I talked to in my unofficial survey of engaged and interested observers of my own pair. I'll paraphrase
If I could get it to recognize someone and provide me with their name when I meet them that would be fantastic!
But it is in urgent care where there is so much potential:
"If I want to look at for example radiology I can double tap ‘radiology...There's his chest x-ray, it just popped up, oh he's got a middle lobe pneumonia"
Part 2 will cover medical applications and how Google Glass technology can be applied in a busy clinical setting